- Speech – normal
- HMF – normal
- Cranial nerves – right facial weakness (including forehead); failure of lateral gaze to right
- ULs – tone normal; power EF 4/5, EE 3/5, distal power 4/5, reflexes brisk on left
- LLs – tone normal; power HF 3/5, HE 5/5, KF 4/5, KE 5/5, reflexes brisk on left
- Sensation intact
Okay, so this does look like a brainstem lesion, and the abrupt onset suggests “vascular” – ischaemic, haemorrhage, AVM etc.
Forehead-involving weakness should be “peripheral” – like in Bell’s palsy – but if you knobble the facial nerve nucleus in the pons, then you get a “lower” looking palsy.
The sixth nerve nucleus controls abduction, and is very close to the seventh. How do I know? Seven comes after six.
So far, so good.
There is an UMN/pyramidal weakness on the left too, so this must be “central”.
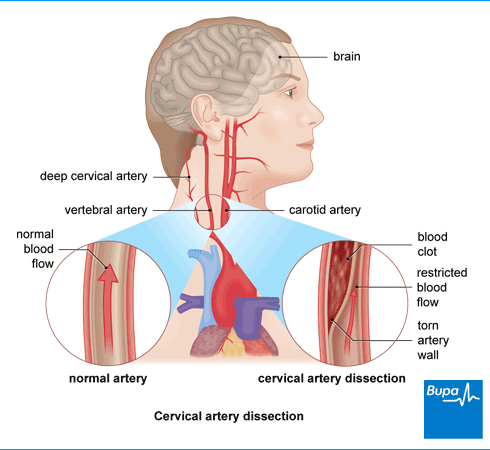
Why would a young man develop a brainstem stroke? Neck pain in this setting is likely to be a vertebral artery dissection. It’s not a rare as you might think, and doesn’t always relate to preceding trauma.
Aside from the usual ABC stuff, and bloods, you are going to want to get an ECG and then a scan of the brain and contrast-enhanced angiography.
CT will rule out a bleed, but MRI will tell you far more.


Speak to the radiologists beforehand and they will (happily) advise on what scans to do.

You might be able to detect that little crescent shape of the affected vertebral artery there. It’s a pretty classical sign for arterial dissection.
The lecture on stroke and TIA gives you a little more on how to approach vascular neurology.
Leave a Reply